- Joined
- 8 May 2010
- Posts
- 1,202
- Reactions
- 0
Very likely true but I suppose it's another example of benefits v risks in consideration of skin cancers. It could be argued that a melanoma is probably a greater risk than osteoporosis.
At least some of the risk of reduced Vit D seems to have been addressed with the addition of Vit D to most of the bone building medications prescribed for osteoporosis.
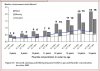
I agree, I was just using it to highlight some evidence of Vit D deficiency.
") , there are many qualifications in the research that we are presented with that the average person isn't aware of and extremists try to gloss over or omit to consider all together.
, there are many qualifications in the research that we are presented with that the average person isn't aware of and extremists try to gloss over or omit to consider all together.